Caregiver Support Groups and Peer Networks
How many caregivers there are and what the role actually costs them The AARP 2023 report counted approximately 48 million U.S. adults providing unpaid care, more than half while…
How many caregivers there are and what the role actually costs them
The AARP 2023 report counted approximately 48 million U.S. adults providing unpaid care, more than half while simultaneously employed. That figure alone should reframe how we think about the workforce, about healthcare, about who absorbs the costs that formal care systems decline to. The Alzheimer's Association's 2025 data adds a more granular lens: dementia caregivers alone contributed an estimated 19.2 billion hours of unpaid care in 2024, valued at $413.5 billion. Those hours don't appear in GDP. The people logging them rarely appear in policy conversations.
The phrase "invisible second patients" has been applied to caregivers, and it holds. The person receiving care has a diagnosis, a chart, a clinical team. The caregiver has a role with no official beginning, no defined scope, and no clear end. Adult children, spouses, working-age adults, rural caregivers in communities with few services: this is not a narrow demographic. It is a diffuse, heterogeneous population united primarily by the sustained, invisible nature of what they carry.
Caregiving is ongoing, not episodic. It doesn't resolve after a hospital stay or a particularly hard month; it compounds. One-time interventions — a single therapy session, a pamphlet from a social worker, a well-meaning conversation with a friend — tend to fall short not because they are poorly designed but because the problem they address is chronic rather than acute. Most interventions available to caregivers were built for crises. Caregiving, mostly, is not a crisis. It is the long accumulation of days in which nothing catastrophic happens and nothing gets easier, either. That distinction shapes what kinds of support actually help, and why.
What burnout actually looks like across emotional, physical, and financial dimensions
A Place for Mom's 2025 survey of more than 1,000 caregivers found that 78% reported experiencing burnout, with many describing it as a weekly or daily occurrence. Stress and anxiety were reported at some point by 87% of respondents; more than half experienced those states at least weekly. The AARP 2023 data found that 56% of caregivers said the role made it difficult to care for their own mental health, and 41% reported feeling lonely.
Burnout does not present in sequence. Disrupted sleep, financial strain, social withdrawal, and emotional depletion arrive together and reinforce one another. A caregiver sleeping four hours a night is less equipped to manage the financial complexity of coordinating care; the financial stress deepens anxiety; the anxiety narrows the social world further. CDC-cited research indicates that approximately one in three dementia caregivers endorses symptoms of clinically significant depression. Not a subgroup statistic. Roughly one in three people doing one of the most demanding jobs in American households, meeting criteria for a diagnosable condition.
The loneliness figure points most directly at what peer support is structurally positioned to address. Loneliness in caregivers is not simply the absence of social contact; it is the more specific experience of feeling unseen, of carrying something that cannot be fully translated to people outside the role. That distinction shapes why peer support differs from a phone call to a friend or an appointment with a therapist — and why the difference is not merely one of degree.
Why peer support works differently than professional help or advice from friends
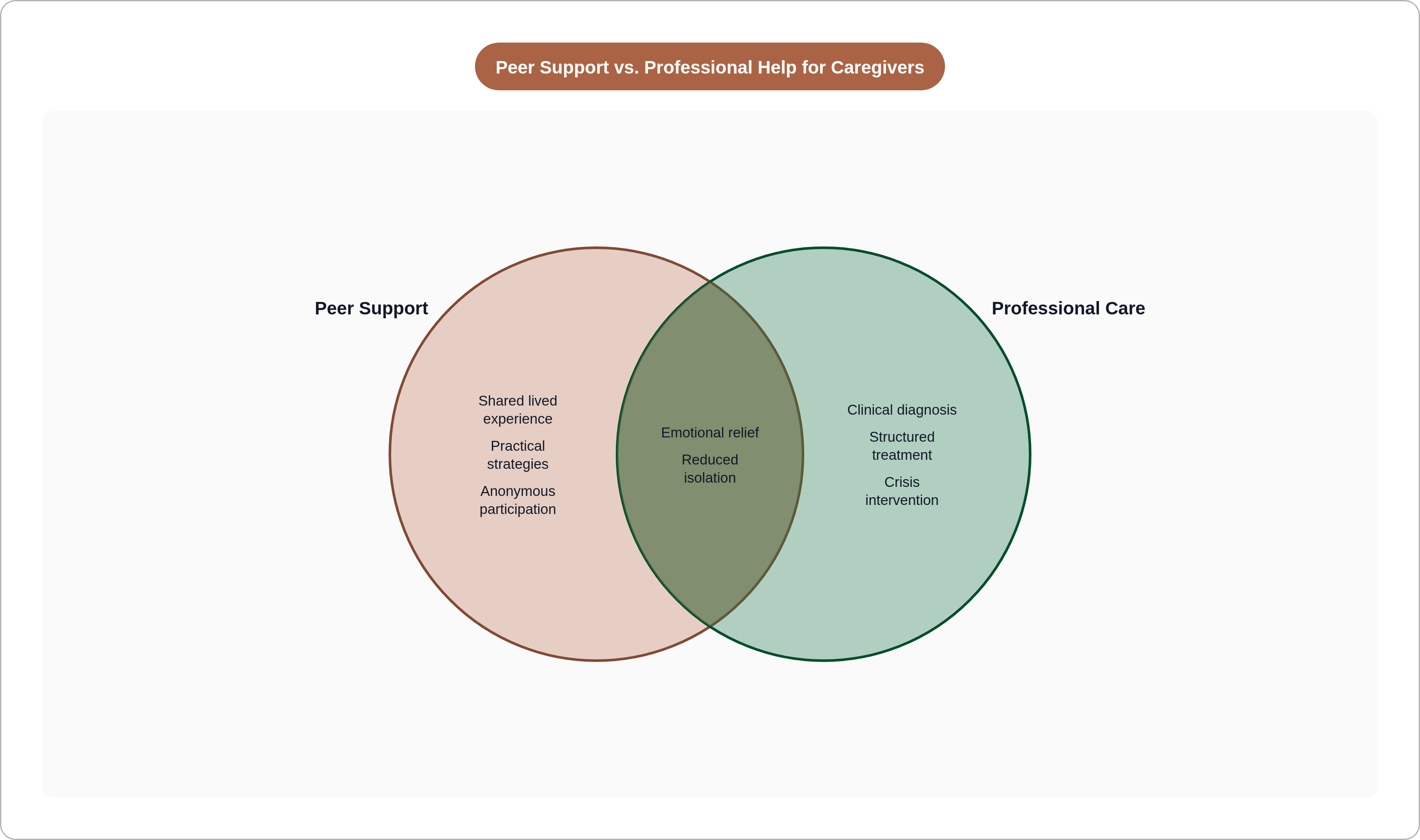
Peer support, defined rigorously, means assistance provided by individuals with shared lived experience, functioning through empathy, mutual recognition, and social connection. It operates through a different mechanism than clinician-led intervention and addresses something a clinical appointment is not designed to reach.
Friends sympathize, often warmly and generously. But sympathy from someone who has never navigated a late-stage dementia diagnosis, never fielded a 3 a.m. behavioral crisis, never tried to balance a full-time job with being the sole decision-maker for a parent's medical care, has a ceiling. In a group composed of people who have done exactly those things, a caregiver doesn't have to explain or justify the guilt, the grief, the ambivalence, the specific texture of the thing. The group already knows. The relief of not having to translate one's experience into terms a listener can understand is, in itself, a therapeutic event — one that professional training doesn't manufacture and friendship rarely provides.
The practical dimension compounds this. Members share strategies: how to navigate a particular hospital system's discharge process, how to manage medication refusals, how to handle aggressive behavior that no one at the neurologist's office had time to address. This is granular, hard-won knowledge that neither a clinician's caseload nor a friend's good intentions can reliably supply.
Online formats introduce an additional variable: anonymity. Caregivers frequently feel pressure to perform competence and optimism, both for the person they care for and for the professionals around them. The option to share difficult emotions without attaching one's name or face lowers the entry barrier considerably. For those not yet ready to share at all, passive participation, reading others' posts, following threads, recognizing one's own experience in someone else's words, appears to be a legitimate and meaningful form of engagement. The ConnectShareCare study, published in JMIR Formative Research in 2025, found that two-thirds of the network's 250 members never posted. Lurking, in the clinical sense, counts.
What the research actually shows about the effects of peer support, and where the evidence stops
The evidence base for caregiver peer support has grown meaningfully in recent years, and reading it honestly means holding the promising findings alongside those that complicate them.
A 2026 meta-analysis of 11 studies involving 1,680 dementia caregivers found that peer support significantly reduced distress, increased perceived social support (SMD 0.37), and improved health-related quality of life (SMD 0.76) post-intervention. Those are not trivial effects. The same analysis, however, found no significant outcomes on depression, anxiety, loneliness, or caregiving burden, and no outcomes showed sustained effects at follow-up. The benefits documented were real; they did not reliably persist.
This is where I think researchers and practitioners tend to reach for reassuring interpretations too quickly. The more uncomfortable question is whether time-limited group studies are even measuring the right thing. A structured group that runs for eight weeks and a sustained peer network that members inhabit for years are not the same intervention. The research hasn't always been careful about that distinction. When the outcome is durability, the design has to be built for duration.
A 2025 meta-analysis by Wei and Han, covering 23 randomized controlled trials, found that community-based supportive interventions significantly improved depressive symptoms, perceived stress, and anxiety among dementia caregivers. A 2024 systematic review of 16 videoconferencing support group studies found that participants across all studies reported the experience as beneficial. A 2023 JMIR scoping review concluded that online support groups generate social support and relieve negative caregiving impacts in ways that parallel the benefits found in face-to-face settings.
Taken together, these findings support a specific and bounded claim: peer support reliably improves social connection and short-term emotional relief. It is not a substitute for clinical treatment of depression or anxiety. A caregiver meeting criteria for major depression needs clinical care; conflating peer support with that care would be a disservice to both. The two approaches are not mutually exclusive, though. A combined model, peer support alongside stress management training and practical caregiving education, may be more robust than any single modality. A 2025 multilevel meta-analysis published in Dementia and Geriatric Cognitive Disorders made precisely that case. The findings are promising, not settled. Long-term outcomes remain underexplored. That gap is a reason to invest in more rigorous follow-up research, not to dismiss what the data already shows.
The main types of caregiver support groups and how they differ
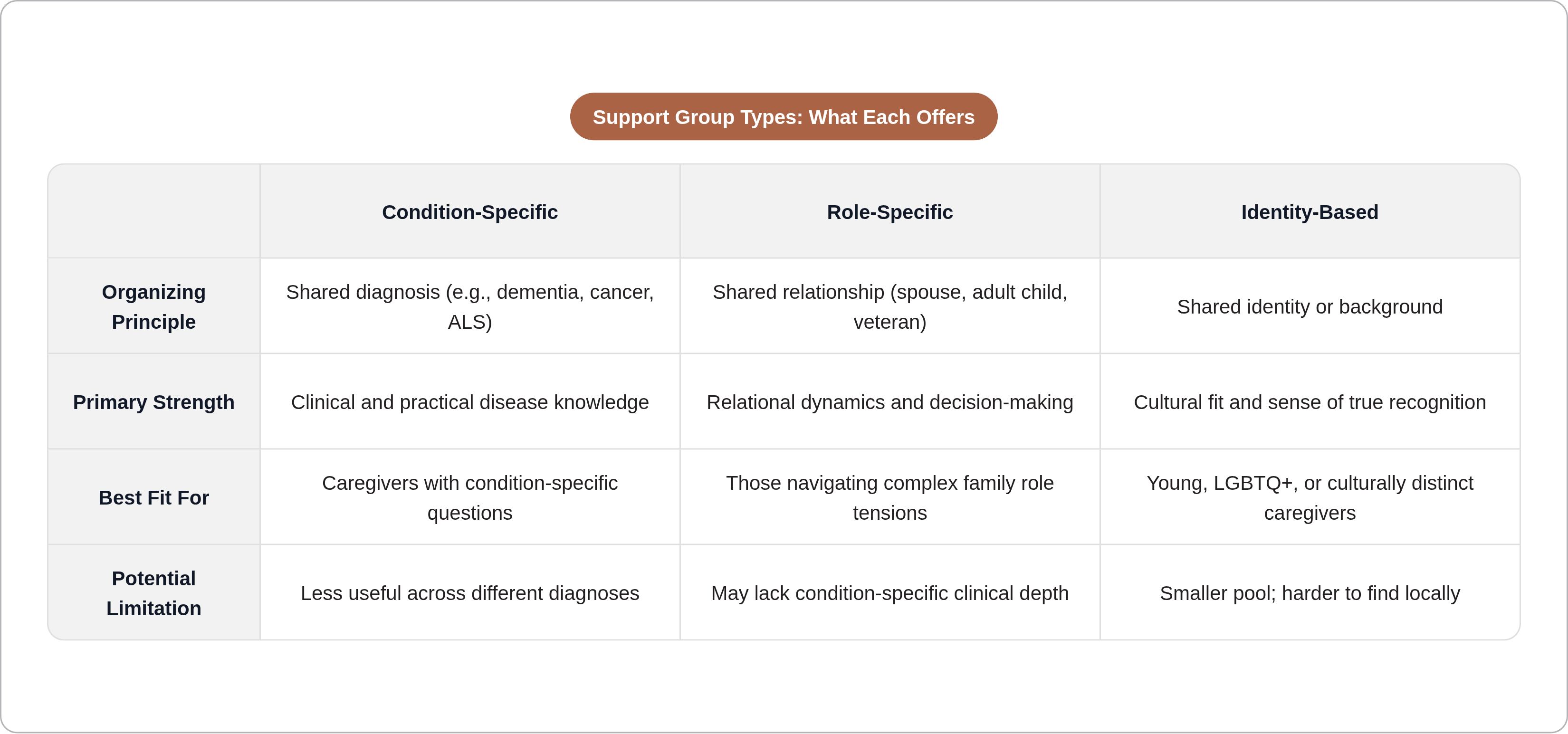
The category "caregiver support group" covers substantial variety, and choosing the wrong type can lead a caregiver to conclude that peer support doesn't work for them when the more accurate conclusion is that a particular group didn't fit their situation.
The most obvious axis is specificity. Condition-specific groups, organized around dementia, cancer, stroke, ALS, or other diagnoses, allow members to share not only emotional experience but highly practical clinical knowledge. A dementia caregiver's questions about behavioral symptoms and legal planning have little overlap with the concerns of a cancer caregiver managing treatment schedules. Role-specific groups, organized around spousal caregivers, adult children, or veteran caregivers, cut differently; they surface shared relational dynamics rather than shared clinical contexts. Both approaches are valid and serve different needs.
Identity-based groups are sometimes dismissed as a niche, but that framing underestimates what they address. Young caregivers navigating a role their peers have no frame of reference for, LGBTQ+ caregivers whose family structures may not be recognized by formal care systems, caregivers from communities where terminology or cultural norms around illness and care differ: these individuals often find generic groups dissonant in ways that reduce rather than increase their sense of being understood. Fit is not a secondary consideration.
The peer-led versus professionally facilitated distinction matters structurally. Peer-led groups offer credibility rooted in shared experience; members know the facilitator has been in the room they're currently standing in. Professionally facilitated groups may provide more structured coping frameworks and clearer guardrails around clinical escalation. It is also worth considering sustainability. A group anchored in a single facilitator who is also an active caregiver carries real burnout risk. Groups with multiple facilitators, supervisory structures, and institutional backing tend to be more durable.
Format is its own dimension: weekly in-person meetings, asynchronous online forums, video calls, private social media groups. Each imposes different participation demands. For many caregivers, the right format is determined less by preference than by circumstance.
Online vs. in-person groups: what each format offers and what it gives up
The case for online groups is primarily one of access. They are available regardless of geography, accessible throughout the week rather than confined to a single meeting window, and they often offer anonymity that in-person settings cannot. One documented online dementia caregiver group grew from 426 attendees in its first year to 914 by 2024, with members joining from 14 states, including rural areas where no local option existed. That growth reflects unmet need.
The case for in-person groups rests on something harder to quantify but not harder to recognize. Physical presence deepens emotional connection in ways that video does not fully replicate. Body language, nonverbal cues, the simple fact of sitting in a room with another person who is also carrying something heavy: these matter, particularly for people already experiencing significant social isolation. Caregivers who have participated in both formats often describe in-person groups as qualitatively different — not superior in every dimension, but irreplaceable in a specific one. That account is worth taking seriously even when it resists measurement.
The Wei and Han 2025 meta-analysis found that both formats produced significant benefits and called for hybrid models as the field matures. Hybrid participation, attending a videoconference group regularly while occasionally joining an in-person group when logistics allow, is a practical arrangement that deserves normalization.
Most caregivers do not choose their format from a menu of options. Rural location, an unpredictable care schedule, an employer with no flexibility, a care recipient who cannot be left alone: these factors make the decision for them. Online access is not a lesser alternative. For a substantial portion of the caregiver population, it is the only alternative, and policy discussions that treat in-person groups as the default and online groups as the accommodation have the hierarchy backward.
Where to actually find a group: national organizations and local starting points
The search goes better when it starts with the condition or role rather than geography. Searching for a dementia caregiver support group is more productive than searching generically, because it surfaces the organizations most likely to connect a caregiver with relevant peers.
Several national organizations offer direct pathways. The AARP Caregiving Resource Center provides tools, articles, and community support for family caregivers broadly. The Caregiver Action Network is a national nonprofit with peer support resources spanning multiple caregiver types and conditions. The Family Caregiver Alliance offers services, education, and advocacy, with particular depth in navigating care systems. The Eldercare Locator connects caregivers to Area Agencies on Aging, a practical bridge to local in-person groups and respite services. The Well Spouse Association provides a national network specifically for spousal caregivers, including an online forum. CaringBridge functions primarily as a communication platform for families navigating a health journey, though it can serve as an entry point to broader peer connection.
Beyond national organizations, hospital social workers are often the fastest path to a condition-specific local group. Geriatric care managers and disease-specific nonprofits, the Alzheimer's Association and the American Cancer Society among them, frequently maintain directories of local groups or run their own. The 211 helpline connects callers to local social services and is chronically underused as a starting point.
Start with the condition or role, identify two or three relevant organizations, and ask directly whether they can connect you to a local or online group. The answer is often yes — and the connection takes minutes.
Barriers that keep caregivers from joining, and how to get past them
Rural caregivers provide an average of eight more hours of care per week than their urban or suburban counterparts and face greater difficulty accessing services, per AARP's 2023 findings. Geographic isolation compounds time poverty in precisely the population with the highest need. The people for whom peer support is most urgent are often the ones for whom it is most structurally out of reach. Any honest account of the model has to contend with that asymmetry.
The most common practical barriers include the absence of a local group, uncertainty about cost, resistance from the care recipient to any outside service involvement, and simple lack of awareness that groups exist. The cost concern is frequently misplaced; many groups are free or low-cost, and disease-specific nonprofits often fund facilitation directly. The awareness gap may be the most addressable of all: primary care physicians, social workers, and hospital discharge planners are logical conduits who remain underutilized in directing caregivers toward peer support.
The time barrier is real but frequently overstated. Asynchronous online forums require no fixed schedule; reading a thread at midnight after the care recipient is settled counts as participation. The hours-per-week commitment need not be large to generate benefit.
Two emotional barriers operate quietly and rarely surface in practical conversations. The first is the belief that caregivers should be coping independently, that seeking peer support signals inadequacy or a failure of commitment to the person they care for. That belief is common, largely unexamined, and unsupported by evidence. The second is discomfort with sharing family information with strangers, which is understandable; naming it as a normal and surmountable hesitation, rather than a disqualifying obstacle, is often enough to move it.
The most consequential barrier may be the "not bad enough yet" threshold. Caregivers frequently wait for a crisis before seeking support. The research suggests that earlier engagement yields more sustained benefit. A support group is not an emergency resource, and it functions better when joined before the emergency arrives.
One practical note: if the first group is not a good fit, that reflects on the group, not on the model. Group culture varies, facilitator quality varies, the demographic and experiential mix of members varies. Switching groups is normal and worth doing rather than abandoning the approach entirely.
What to expect when joining a group and how to get more out of it
The first meeting is frequently disorienting. The group has its own language, its own reference points, its own unspoken norms developed over months or years of shared experience. Listening before sharing is not only a reasonable approach; it is often the one that leads to more meaningful eventual participation.
The ConnectShareCare finding that two-thirds of members never posted does not reflect a failure of those members. Passive participation — reading, observing, recognizing oneself in another person's account — is documented and legitimate. For many caregivers, that level of engagement is what they can manage, and it appears to generate real benefit. For those who eventually move toward active sharing, the evidence suggests that giving and receiving support are not cleanly separable; caregivers who contribute their own experience to the group tend to report deeper benefit than those who only receive.
A support group is not a mental health treatment. If depression or anxiety symptoms are clinically significant, peer support and professional care should coexist, not compete. A well-functioning group will recognize this and, ideally, facilitate referrals when members appear to need more than the group can provide.
Signs that a group is working: a reduced sense of isolation, practical information that translated into a real change in how a specific situation was handled, the experience of feeling understood rather than assessed. Signs to look elsewhere: advice that consistently mismatches the caregiver's situation, an absence of any facilitation structure, group dynamics that leave members more depleted than they arrived.
One benefit that rarely appears in clinical research but surfaces consistently in caregivers' own accounts deserves mention. Peer networks are frequently where caregivers first learn about financial assistance programs, benefits, and services they didn't know they qualified for. Members share that information informally, without professional gatekeeping, and with the specificity that comes from having navigated the system themselves. For a population managing the financial weight that the AARP and Alzheimer's Association data makes visible, that knowledge transfer is not incidental to the support — it is often the most immediately useful thing that happens in the room.